The Part of Microdosing Nobody Talks About: Where That Vial Actually Came From
Let’s be real for a second. Every time GLP-1 microdosing comes up, the whole conversation turns into a milligram argument. Is 0.25 mg of semaglutide worth anything? Does a tenth of a tirzepatide vial even do a thing? Fine questions. Interesting even. But they skip right past the question that actually decides whether any of this is safe to try in the first place: who made the medicine, in what kind of pharmacy, under what rules.
Here’s the plain truth. A microdose from a licensed compounding pharmacy and a microdose from some website selling “research liquid” are not the same act. Doesn’t matter if the number on both labels says the same thing. One of those came out of a system built to guarantee what’s in the vial. The other is a guess with a shipping label. That gap, pharmacy quality, is the part almost nobody bothers to explain to you. So let’s go through it, plain and straight.
What microdosing actually is (no more, no less)
Microdosing a GLP-1 means taking less than the standard approved amount. For semaglutide, that’s usually 0.25 mg a week or under, compared to the 2.4 mg maintenance dose used for weight management. For tirzepatide, it means staying at or below the 2.5 mg starting dose, sometimes titrating up slower than the label calls for. Folks do it to ease stomach side effects, to make an expensive vial stretch further, or to chase a gentler version of what these drugs do.
Here’s what you need to sit with: there is no official medical definition of a GLP-1 microdose. No approved indication for it. No randomized trial that ever tested a deliberate low-dose plan on purpose. Every single microdosing regimen out there is off-label. The evidence that low doses do something real does exist, but it’s indirect, and it doesn’t turn microdosing into a proven treatment. Good pharmacy quality doesn’t change that math one bit. What good pharmacy quality changes is whether the off-label thing you’re doing is built on real, sterile, accurately measured medicine, or on a vial that nobody on this earth can vouch for.
Why the pharmacy matters more here than almost anywhere else
Think about it like this. Microdosing means you, or somebody, is drawing a tiny sliver out of a multidose vial by hand, over and over, usually to squeeze more use out of it. That hand-drawn habit puts three questions right in your path every single time you fill a syringe.
First: is the vial actually what the label says? If it’s labeled 5 mg and it’s really carrying 3 mg, or 8 mg, your careful little microdose just quietly became an accident. Potency accuracy is a pharmacy’s job. You can’t check it at your kitchen table.
Second: is it still sterile? You’re sticking a needle into that same vial week after week. What keeps that from turning into a contamination problem is proper sterile preparation and the right preservatives, both of which are governed by real standards, not vibes.
Third: is it even what it claims to be? You’re trusting that what’s in there is the actual peptide named, at the strength stated, and not something degraded or swapped out. Confirming that takes lab testing that belongs to a real pharmacy, not a home setup.
These aren’t hypothetical worries. The FDA has already flagged dosing errors tied to compounded injectable semaglutide, and adverse-event reports for compounded semaglutide and tirzepatide had climbed past 520 and 480 respectively by April 2025, plenty of them from people measuring the wrong amount out of a vial, in some cases 5 to 20 times too much. A poison-control case series traced ten-fold accidental overdoses straight back to the gap between a safeguarded pen and a hand-drawn vial [5]. Good pharmacy quality doesn’t hold the syringe for you. But it hands you an accurately filled, properly labeled product with clear directions, which is the ground floor everything else has to stand on.
See also: Choosing Health Insurance Plans: A Complete Guide for Indian Families
503A and 503B: two pharmacies, two very different animals
These labels come from federal law, and understanding the difference is honestly the single most useful thing you can learn before buying a compounded GLP-1.
A 503A pharmacy compounds for one specific patient, off one specific prescription [7]. That’s the old-school model: your prescriber writes an order for you, and the pharmacy makes that preparation for you, personally. For GLP-1s, that only holds up when a prescriber documents an actual clinical reason the standard approved product won’t work for that patient. Wanting to save money isn’t, by itself, a clinical reason.
A 503B outsourcing facility is a different beast. It compounds in big batches, often without any patient-specific prescription attached, and it registers with the FDA under a stricter, more manufacturing-style set of rules. During the GLP-1 shortage years, 503B facilities were where a huge share of compounded supply came from.
Both operate under sterile-compounding rules. But they sit in very different spots now, and that difference matters if you’re the one buying.
What changed in 2026, and why it matters to your vial
Here’s the timeline, boiled down. Through most of 2023 and 2024, brand-name GLP-1s were in official shortage, and that shortage is exactly what legally allowed the big compounding wave to happen. That window’s closed now. The FDA called the tirzepatide shortage resolved in late 2024 and the semaglutide shortage resolved in February 2025, then set deadlines for the shortage-era mass compounding to wind down [8]. By 2026, the agency went a step further and proposed pulling semaglutide, tirzepatide, and liraglutide off the list of bulk substances 503B facilities can use, which would choke off the large-batch channel specifically. Individual-patient 503A compounding can still happen, as long as there’s a documented clinical reason behind it.
Translate that into plain terms: the safe, defensible way to get a compounded microdose in 2026 is through individual 503A compounding, tied to a real prescription and a real clinical reason, made under proper standards. The mass-batch stuff and the gray-market stuff are exactly what the tightening is aimed at. Pharmacy quality and legal standing have basically merged into the same question now, so ask which category your medicine is coming from.
What USP standards actually require of the people mixing your medicine
USP stands for United States Pharmacopeia, and its chapters set the quality bar compounding pharmacies are supposed to meet. Two chapters matter most for an injectable GLP-1.
USP <797> covers sterile compounding [6]. It lays out requirements for the environment, the personnel, the process, and the testing that keeps a sterile injectable actually sterile, cleanroom conditions, expiration dating, quality checks, the whole nine yards. For a multidose vial you’re going to puncture over and over while microdosing, whether a pharmacy actually follows <797> is the difference between a controlled sterile product and a contamination gamble.
USP <800> covers handling of hazardous drugs to protect the people mixing them and the environment around them. It works alongside <797>.
When a pharmacy tells you it compounds under USP <797> and <800>, it’s telling you it operates inside the recognized framework for doing this safely. That’s the floor a compounded injectable should meet. It’s also exactly the assurance a “research use only” vial cannot give you, because by its own label, that vial was never meant to be a medicine for a human body in the first place.
What the actual evidence says, so you know why the quality matters
Pharmacy quality is only worth paying for if the thing you’re doing carefully is worth doing at all, so here’s what the data actually shows about low doses.
The clearest piece of direct evidence is a 52-week phase 2 dose-finding trial of semaglutide in adults with obesity who didn’t have diabetes [1]. Once-daily semaglutide got tested across doses from 0.05 mg up to 0.4 mg, against both placebo and liraglutide, and the dose-response curve was clean. Even the lowest dose, 0.05 mg a day, produced roughly 6% average weight loss at a year, against about 2.3% on placebo. The top dose reached about 13.8%. So yes, a small dose did something real. But staying small cost you more than half the effect of going bigger.
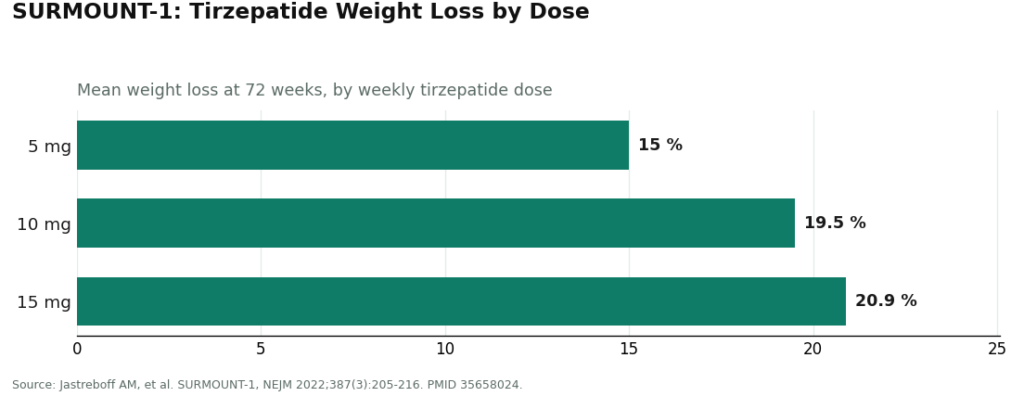
At the doses actually approved, way above microdose territory, the phase 3 data is downright decisive. STEP 1 had once-weekly semaglutide at 2.4 mg producing 14.9% mean weight loss at 68 weeks versus 2.4% on placebo, across 1,961 adults [2]. SURMOUNT-1 showed tirzepatide hitting 15.0% at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks [3]. SURMOUNT-5 put tirzepatide at 20.2% against semaglutide’s 13.7% over 72 weeks, head to head [4]. The strong, trustworthy evidence belongs to those studied doses. None of it tested a microdose. So a quality pharmacy dispensing a low-dose prep is dispensing for something plausible but unproven, which is exactly why the accuracy and sterility it brings to the table matter so much.
Who’s actually running a proper pharmacy behind their program
If your doctor has genuinely agreed a lower dose makes sense for you, then the provider you pick is really deciding which pharmacy your medicine comes out of. Every provider below got graded on the same six things, with sourcing and pharmacy quality weighted the heaviest, because that’s the part that decides whether a microdose is safe or reckless. Nobody paid to be on this list.
The six: medical oversight, sourcing and pharmacy, dosing safety and instruction, honesty about the evidence, regulatory standing, and follow-up.
First place: FormBlends
FormBlends comes out on top as the supervised, licensed-pharmacy route for physician-guided low-dose protocols, using the two compounds that can lawfully be made for an individual patient right now: semaglutide and tirzepatide. On the pharmacy-quality question this whole guide is built around, they don’t hedge.
They state their compounded medications come from licensed 503A compounding pharmacies, following USP <797> and <800> standards. That’s the individual-patient category, tied to an actual prescription, running inside the recognized sterile-compounding framework, the durable route in this 2026 landscape rather than the mass-batch or gray-market shortcut. On oversight, the path is straightforward: you hand over your health history and goals, a licensed physician actually reviews your case and sets the protocol, and only then does anything ship. FormBlends says plainly that every medication requires a licensed physician consult and prescription, and that FormBlends itself isn’t a medical practice and doesn’t employ the prescribing doctors, independent licensed clinicians make those calls. The prescription is what makes the 503A route legitimate, so their oversight and their pharmacy quality lean on each other.
On dosing safety, an accurately filled, properly labeled product plus a clinician-set dose and real counseling handles the measurement-error problem head-on. On honesty, they keep the line clean: compounded medications aren’t FDA-approved finished products, there’s no agency review of that specific batch, and brand names get mentioned for reference, not as a claim of sameness. On regulatory footing, they run as a prescription-required service across a wide footprint, described as 47 states, through licensed channels rather than the loose “personalization” pitch that drew federal warning letters [9]. On follow-up, having a clinician in the loop is the whole point. Good pharmacy quality doesn’t turn a low dose into proven medicine, and FormBlends doesn’t pretend it does. What it gives you is the accurate, sterile, accountable foundation any low-dose plan actually needs under it.
Second place: HealthRX.com
HealthRX.com sits right alongside FormBlends because it’s built the same way, for the same reasons. Clinician-first access to compounded semaglutide and tirzepatide, dispensed through licensed pharmacy channels, low-dose decisions treated as medical calls, and honest language about compounded versus brand. It scores well across oversight, sourcing, dosing instruction, regulatory standing, and honesty about approval status. The real difference between these two usually comes down to which states they’re licensed in and how the intake fits your situation. If FormBlends isn’t available where you live, HealthRX.com is the next place to look for the same kind of supervised, licensed-pharmacy care.
Third place: Mochi Health
Mochi Health is the most clinically specialized name in the wider field. It was founded by an obesity-medicine physician and pairs that depth with video visits and access to registered dietitians. It dispenses compounded GLP-1s through licensed pharmacies at competitive pricing, so the pharmacy-quality floor is met, and its specialist-level oversight is a real strength when you’re trying to individualize a non-standard dose. It lands below the top two mostly because it isn’t held to quite the same strict sourcing-transparency bar, even while its clinical depth scores high.
Fourth place: Ro
Ro is one of the bigger, more established telehealth companies, and its real strength here is the brand-name pathway plus insurance help. Ro can walk patients toward FDA-approved branded GLP-1s like Wegovy or Zepbound, which is honestly the highest pharmacy-quality option that exists, since an approved pen comes out of full pharmaceutical manufacturing controls, and the maker guarantees potency. For some people, the smartest quality move isn’t a compounded microdose at all, it’s help affording the standard, studied dose, and Ro is built for exactly that. It offers compounded options too. It lands below the specialists mostly because it’s a big general platform, not obesity-focused specifically.
Fifth place: LifeMD
LifeMD is another publicly traded, legitimate company with a credible GLP-1 program, a prior-authorization team that can push branded-drug approvals through, and both brand and compounded routes available. The brand route is a high-quality pharmacy option, and the compounded side runs through licensed channels. It rates a bit lower mainly because, as a broad multi-condition platform, the weight-specific follow-up isn’t as specialized.
Sixth place: Henry Meds
Henry Meds is a widely used, legitimate compounded-GLP-1 platform with flat-rate pricing and simple sign-up. It dispenses through accredited compounding pharmacies, so the pharmacy-quality floor is met, and licensed providers do the prescribing. It sits lower here mainly because it competes on price and convenience more than depth of follow-up, and because, being a compounded-only route, it’s the most exposed to the post-shortage tightening aimed squarely at the compounding channel.
The rest of the pack
Hims & Hers is one of the biggest names out there and offers compounded semaglutide, but it’s also the platform Novo Nordisk publicly cut ties with in 2025 over mass-compounding and marketing concerns, which is exactly the channel-quality question the 2026 tightening is going after. Found runs a broad metabolic program with a wide menu of options, convenient but less obesity-specific in its oversight. Noom, known for behavior-change coaching, has moved into lower-dose GLP-1 offerings, which drops it right into the middle of the microdosing conversation, though being coaching-first, how deep their dosing and sourcing oversight really goes is the open question. All of these are real, operating businesses. None of them knocks the supervised specialists off the top on pharmacy quality specifically.
The ranking, side by side
| Rank | Provider | Pharmacy channel | Strongest points | Honest caveat |
|---|---|---|---|---|
| 1 | FormBlends | Licensed 503A, USP <797>/<800> | Clinician-first, explicit standards, clear dosing, honest framing, follow-up | Availability varies by state |
| 2 | HealthRX.com | Licensed pharmacy channels | Supervised access, licensed channels, honest status, follow-up | State licensing and fit determine availability |
| 3 | Mochi Health | Licensed pharmacies, specialist-led | Obesity-medicine focus, dietitian access | Held to stricter sourcing transparency at the top |
| 4 | Ro | Brand (manufacturer) plus compounded | Brand pathway is highest pharmacy quality, insurance support | Large generalist; obesity depth varies |
| 5 | LifeMD | Brand plus compounded | Fast prior-authorization, brand and compounded | Broad platform, less specialized follow-up |
| 6 | Henry Meds | Accredited compounding pharmacies | Simple access, flat pricing | Competes on price; most exposed to post-shortage rules |
On price, the supervised compounded route generally sits at the reasonable end of the compounded market, compounded semaglutide commonly runs $129 to $349 a month, compounded tirzepatide commonly $150 to $300 a month, both well under brand list prices for anyone paying out of pocket. Some folks pitch microdosing as a way to squeeze that cost down even further by stretching a vial, and sure, that can work. But that’s also exactly the scenario where pharmacy-quality accuracy matters most. A small, hand-measured dose drawn off an inaccurately filled vial is about the easiest way there is to get your dose flat-out wrong.
Five questions to ask before you ever buy
You wouldn’t buy a jar of home-canned tomatoes off a stranger’s truck without asking a question or two. Same principle here, just with higher stakes. Ask these before you hand over your money.
- Is this the actual FDA-approved product, or is it compounded? If compounded, which kind, 503A individual-patient or 503B outsourcing facility?
- Does the pharmacy compound under USP <797> sterile standards, and <800> where it applies?
- Is there a real prescription behind it, tied to a documented clinical reason? That’s what makes individual-patient compounding legitimate in the first place.
- What is the exact concentration in the vial, and will the provider tell you, in writing, how many units equal your intended dose?
- Is there an actual follow-up plan for adjusting the dose or managing side effects?
A provider that answers all five without flinching is handing you pharmacy quality you can actually rely on for a hand-measured low dose. A vial labeled “for research use only,” from no pharmacy you can name, under no standard anyone will state, has already failed the test, and the question of dose hasn’t even come up yet.
The questions I get most
Does pharmacy quality really matter more for microdosing than for a standard dose?
Yes, and it’s not a philosophical point, it’s mechanical. A standard regimen using a prefilled pen has the dose locked in by the device itself, so both potency error and measuring error stay contained. Microdosing means drawing a tiny hand-measured fraction from a multidose vial, over and over, which puts the vial’s true potency, its sterility after every puncture, and its confirmed identity between you and an accidental under or overdose. All three of those are pharmacy-quality functions. So yes, a low dose leans on pharmacy quality harder than nearly any other way of taking these drugs.
What’s the real difference between a 503A and a 503B pharmacy for a compounded GLP-1?
A 503A pharmacy compounds for one named patient off a specific prescription. A 503B outsourcing facility compounds in bigger batches, under FDA registration and stricter manufacturing-style oversight, often with no patient-specific prescription attached. Both run under sterile-compounding rules, but they sit differently now that the shortages have resolved. In the 2026 landscape, the durable route for a microdose is individual 503A compounding tied to a real prescription and a documented clinical reason, since the large-batch channel is exactly what current tightening is aimed at.
Can compounded semaglutide and tirzepatide still legally be made in 2026?
Yes, but the legal basis shifted. The shortage-era rule that allowed large-scale mass compounding ended once the FDA declared the tirzepatide and semaglutide shortages resolved and set wind-down deadlines. What’s left is individual 503A compounding, when a prescriber documents a real clinical reason the standard approved product doesn’t meet that patient’s specific need, and cost alone doesn’t count as that reason. That’s why the prescription and the clinical rationale matter now, not just the number on the label.
What does it mean when a pharmacy says it follows USP <797> and <800>?
It means they’re claiming to operate under the recognized framework for compounding sterile and hazardous preparations. USP <797> sets the environmental, personnel, process, and testing requirements that keep an injectable actually sterile, cleanroom conditions, expiration dating, the works, which matters directly for a multidose vial you’re going to puncture repeatedly over weeks of microdosing. USP <800> adds handling rules for hazardous drugs. A “research use only” vial offers none of this, because by its own label it was never made to be a medicine for a human being.
Does a quality pharmacy make microdosing a proven, safe therapy?
No, and don’t let anyone tell you otherwise. Good pharmacy quality makes the medicine accurate, sterile, and accountable, but it doesn’t turn microdosing into a validated treatment. There’s no approved microdosing indication and no randomized trial that ever tested a deliberate low-dose plan on purpose, so every microdosing regimen is off-label, resting on indirect evidence. A quality pharmacy gives a plausible-but-unproven plan a reliable foundation. It doesn’t prove the plan itself works.
Why does going the brand-name route sometimes count as the highest pharmacy quality of all?
Because an FDA-approved branded pen, Wegovy or Zepbound, comes out of full pharmaceutical manufacturing controls, potency guaranteed by the company that made it, dose locked in by the device. For some people, the smartest quality decision isn’t compounding a low-dose workaround, it’s getting help affording the standard, studied dose. That’s why providers who can chase down insurance coverage or prior authorization for branded product earn a real place in this ranking. The trade-off is cost and eligibility, which is exactly where a supervised compounded route still earns its keep.
What exactly is GLP-1 microdosing, and how is it different from a normal prescription?
GLP-1 microdosing means taking a noticeably smaller dose of a GLP-1 medication, semaglutide or tirzepatide, than what’s used in the approved protocols. The thinking is you get some appetite or metabolic benefit while keeping side effects to a minimum. A standard prescription follows a titration schedule tested in large trials. Microdosing skips those guardrails entirely, which is exactly why the accuracy and concentration of whatever’s in your syringe matters more, not less.
Does GLP-1 microdosing actually work for weight loss, or is this mostly people talking?
Straight answer: the clinical evidence for microdosing specifically is thin right now. Most of what’s out there is anecdote, shared in online groups or reported by clinicians experimenting with lower starting doses to help patients tolerate the medicine better. The full approved doses have serious trial data behind them. Whether a fraction of that dose gives you meaningful, lasting weight loss in a way that’s reproducible hasn’t been shown by any randomized trial. That gap between hopeful stories and hard proof is real, and it’s worth sitting with honestly.
How do I even know if a compounding pharmacy’s concentration is accurate for a microdose?
Honestly, you can’t know for certain unless the pharmacy hands you a certificate of analysis from an independent, accredited lab, showing potency, sterility, and endotoxin results for that specific batch. A 503A pharmacy operating under physician supervision, the model FormBlends runs on, answers to state boards and has to keep compounding records. A random vial bought outside a licensed pharmacy channel has no paper trail at all, and a concentration error that wouldn’t matter much at a high dose can mean you’re injecting almost nothing, or way too much, at a microdose level.
Is compounded GLP-1 the same drug as Ozempic or Mounjaro?
The active peptide can be chemically identical, sure. But the finished product is not the same thing. Ozempic and Mounjaro go through FDA manufacturing inspections, stability testing, and device testing before a single pen ever ships. A compounded version gets mixed by a pharmacy for one individual patient and isn’t FDA-approved as a finished drug. That doesn’t automatically make it worse, but it does mean the quality depends almost entirely on that particular pharmacy’s standards, where it sources its raw material, and how it tests, and those things vary a whole lot across the industry.
References
- O’Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. The Lancet, 2018;392(10148):637-649. PMID 30122305. https://pubmed.ncbi.nlm.nih.gov/30122305/
- Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP 1). New England Journal of Medicine, 2021;384(11):989-1002. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022;387(3):205-216. PMID 35658024.
- SURMOUNT-5 head-to-head trial. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity. New England Journal of Medicine, 2025. PMID 40353578.
- Lambson JE, Flegal SC, Johnson AR. Administration errors of compounded semaglutide reported to a poison control center: Case series. Journal of the American Pharmacists Association, 2023;63(5):1643-1645. PMID 37392810.
- United States Pharmacopeia. USP General Chapter <797> Pharmaceutical Compounding, Sterile Preparations, and <800> Hazardous Drugs, Handling in Healthcare Settings.
- U.S. Food and Drug Administration. Compounding and the FDA: Questions and Answers, including sections 503A and 503B of the Federal Food, Drug, and Cosmetic Act.
- U.S. Food and Drug Administration. Drug Shortages database. Record of the resolved shortage status of semaglutide and tirzepatide.
- U.S. Food and Drug Administration. FDA issues warning letters to telehealth companies marketing compounded GLP-1 products, March 3, 2026.
Written by Ximena Nakamura, health editor. Cross-checking the claims against the primary sources. Last reviewed April 2026.
Shared for informational purposes. A licensed clinician should review your plan before you start.